Hearing Aid Styles and Fitting Applications
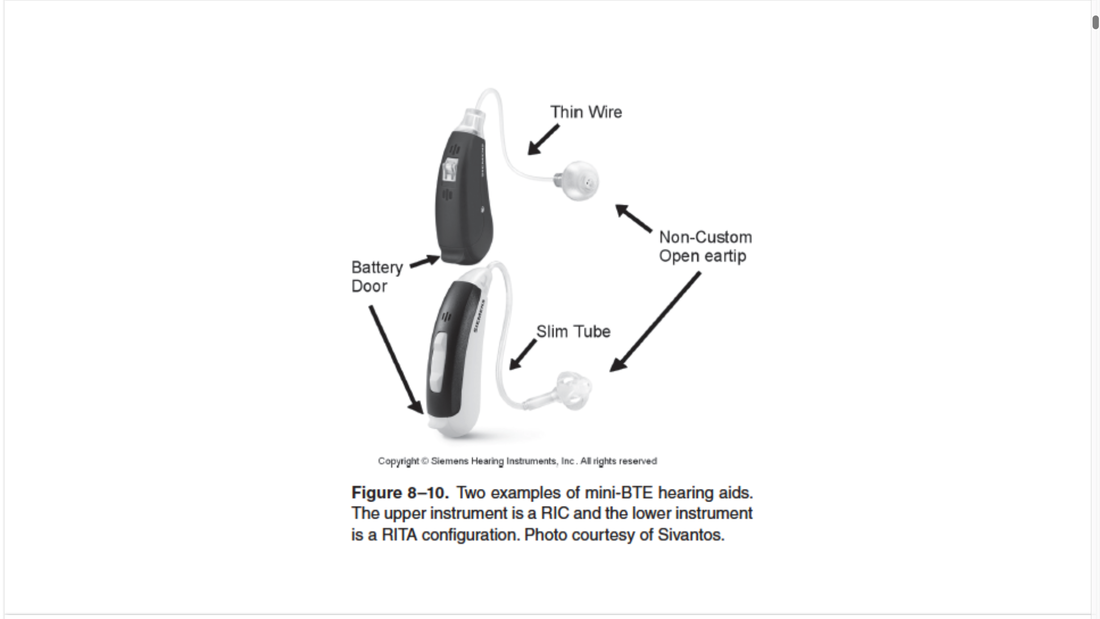
MINI-BTEs (mini behind the ear)
- a more recent incarnation of the traditional BTE instrument is the mini-BTE hearing aid
- significantly smaller than traditional BTEs but do fit behind the ear
- can be fitted in several different ways but fall into two general categories
- RITA
- configured like a traditional BTE except the case is smaller meaning that a smaller batter is necessary
- shorter batter life, typically less power
- uses very thin tubing to transmit the signal to the ear
- unlike standard #13 tubing used by most traditional BTEs
- there is no earhook, the tubing is attached directly to the BTE case
- configured like a traditional BTE except the case is smaller meaning that a smaller batter is necessary
- RIC
- small BTE case which is coupled to a thin wire that attaches to a small external receiver that is placed in the ear canal
- receiver is then coupled to the ear using a custom or non-custom eartip
- advantage of the RIC over the RITA is that because the receiver is removed from the case, the case can be made somewhat smaller and more unique designs can be implemented
- larger receivers can be coupled to the hearing aid to provide more power than usually available with a mini RITA
- RITA
- The larger size of the traditional BTE case also makes it possible to apply various other technologies, including
- derectional microphones
- wireless signal routing
- strong telecoils
- direct auditory input
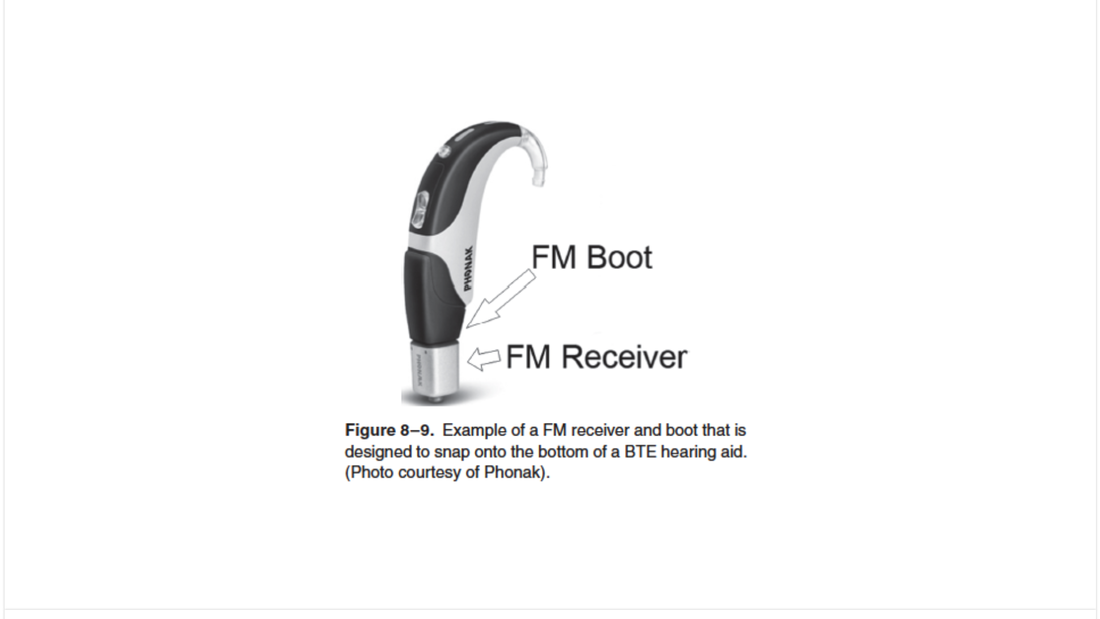
- Improved miniaturization has also allowed for frequency modulated (FM) receivers to be attached directly to a BTE via a boot
- with FM, the carrier frequency can be modulated by the analog signal of interest
- one strong advantage to FM compared to some other analog transmission methods is that even when there is a weak carrier signal, the embedded signal of interest is still preserved
- with an FM system you can hook up a number of things
- can be a lanyard or clip on a microphone, like a heavy duty microphone
- can have bluetooth and then transmit it via FM
- we see less of these as we start to get more streamlined small things that patients are using elsewhere]
- are often maintained by school systems that have a dedicated audiologist
- in California, there is maybe one per county
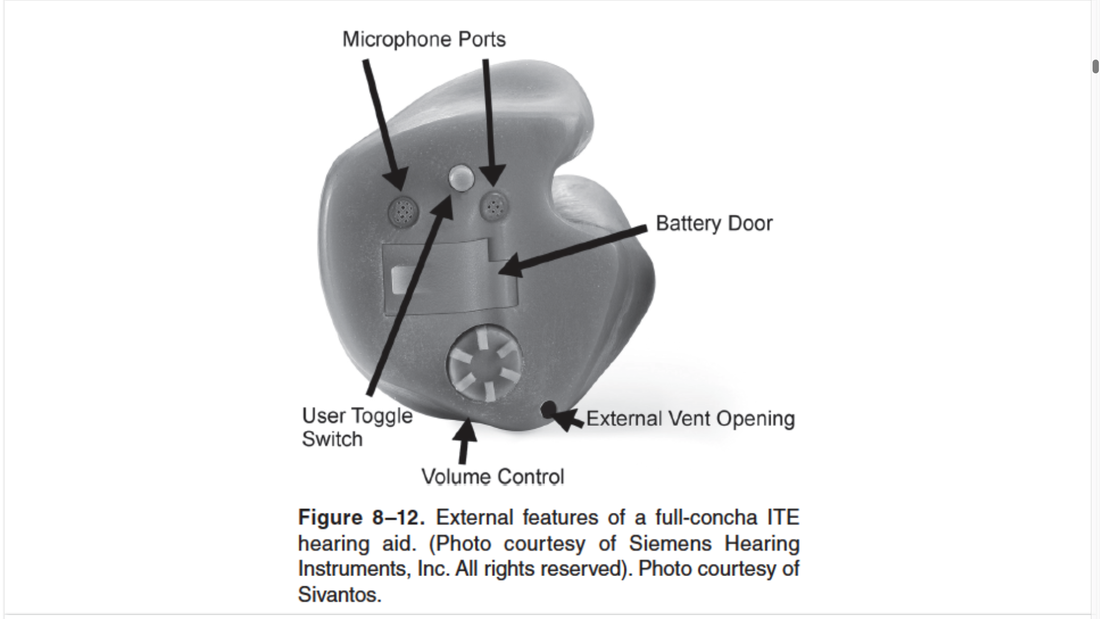
ITE (In the ear)
- multiple microphone ports
- external vent opening
- volume control
- etcetera
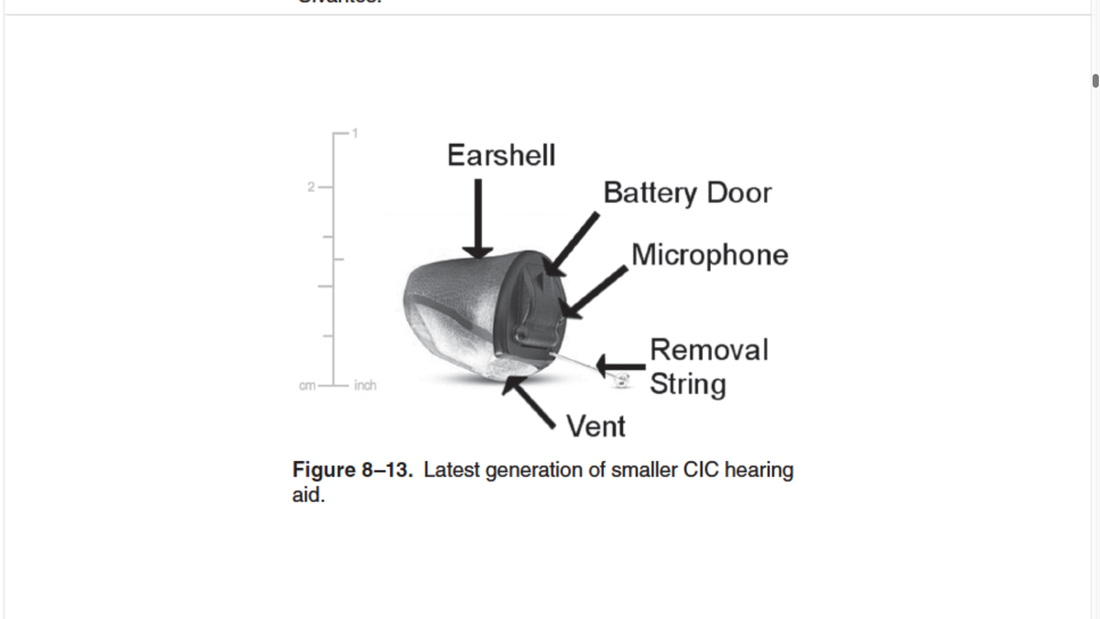
CIC
- Completely In the Canal
Bone Conduction Stimulation
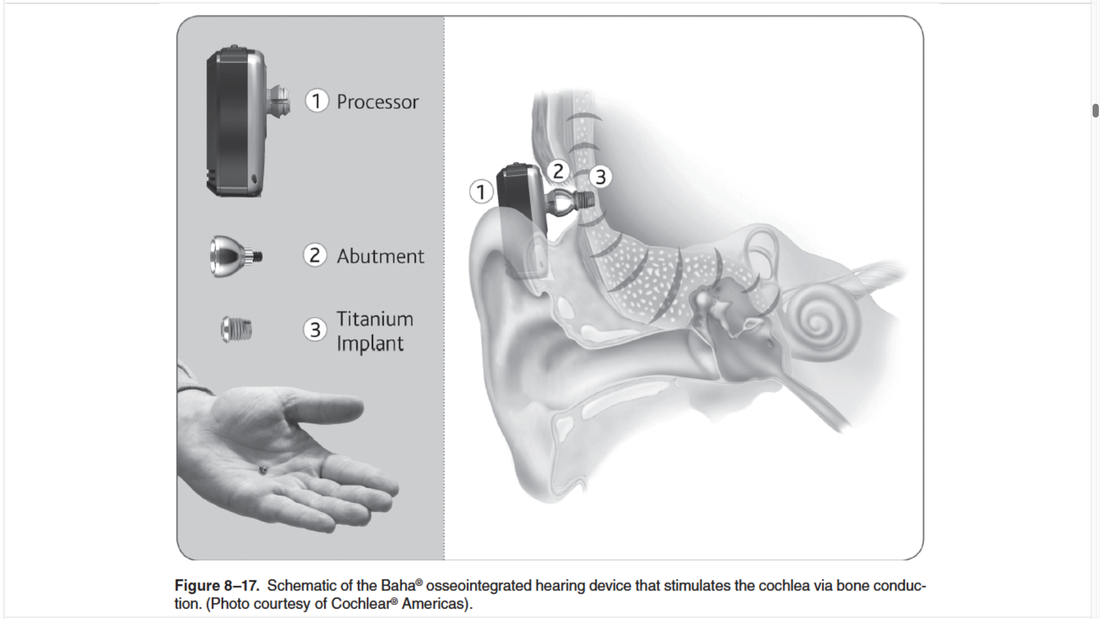
- Ahah osseo-integrated hearing device that stimulates the cochlea via bone conduction
- initially designed for individuals with conductive hearing losses
- consist of an externally mounted processor connected to an abutment and a titanium implant that is attached to the skull
Middle Ear Implant
- developed for patients who have sensorineural hearing loss and are usually thought of as candidates for traditional air conduction hearing aids
- when would you recommend a cochlear implant?
- when have spiral ganglion cells
- for someone who has no hearing as the insertion of this device essentially destroys the cochlea
- someone would have to have severe to profound hearing loss and their speech understanding would be lacking
- Hybrid
- essentially an implant that is inserted in the cochlea part of the way and has a hearing aid function for the rest of the way
- for someone with dead regions, especially high frequency loss because would be inserted from base to apex (high frequency to low frequency)
- precipitous high frequency
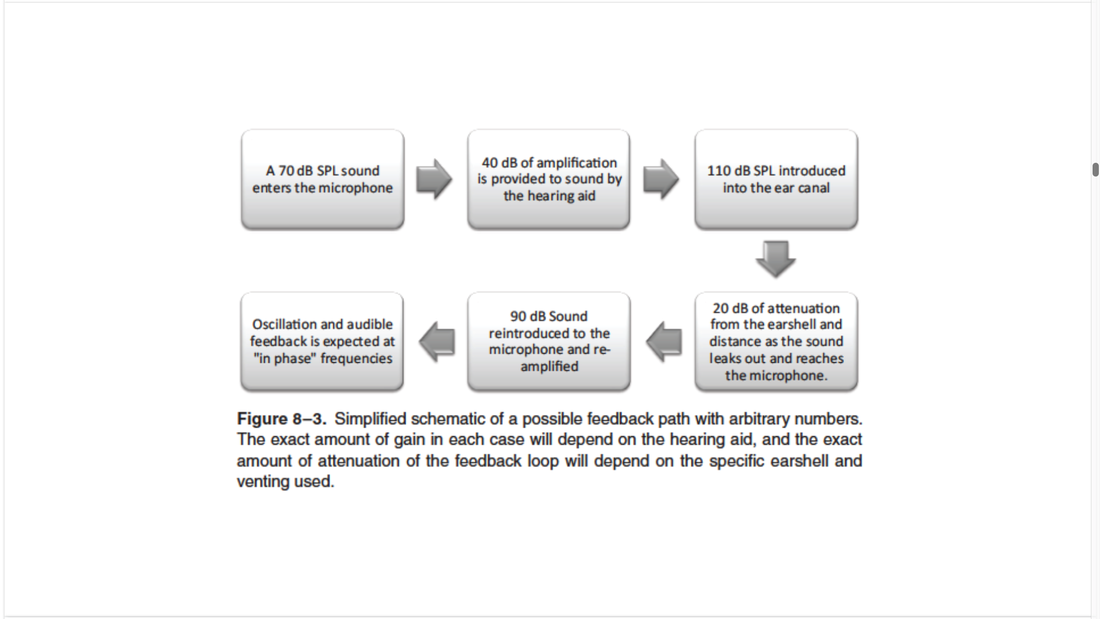
Acoustic Feedback
- occurs when amplified sound from the receiver finds a pathway back to the microphone and is re-amplified by the hearing aid repetitively in a feedback loop
- the attenuation of the shell can cause feedback
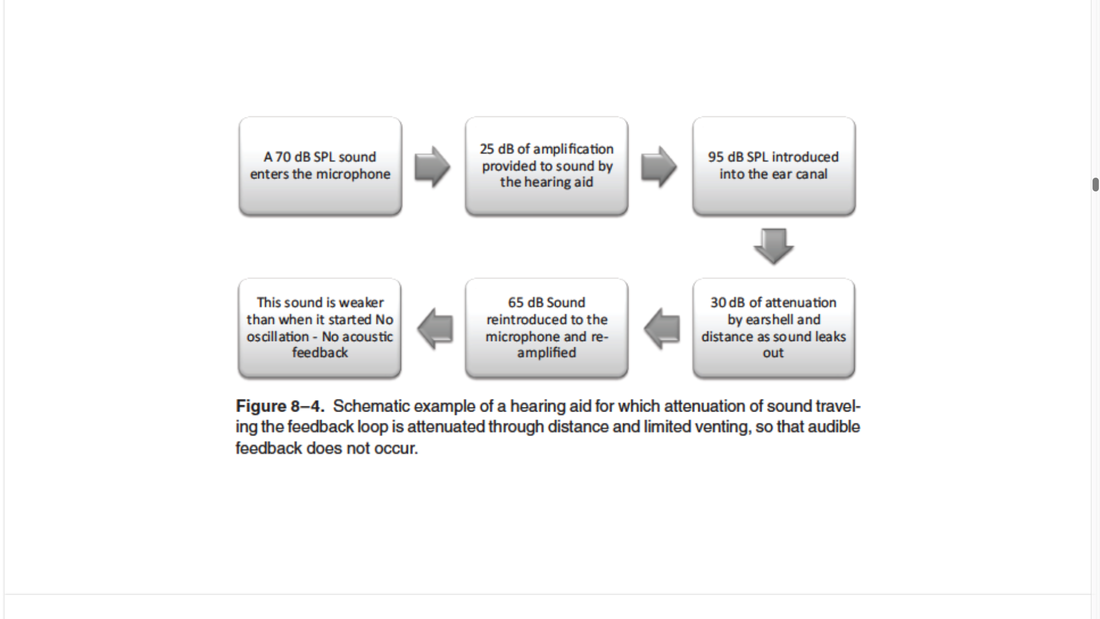
- creating more attenuation can reduce this by closing the vent and preventing the signal from flowing back out!
- If we have a loose fit @ 95dB in the canal and 10dB outside then the attenuation is 85dB
- the higher the attenuation then the less chance of feedback
Critical Gain Measures
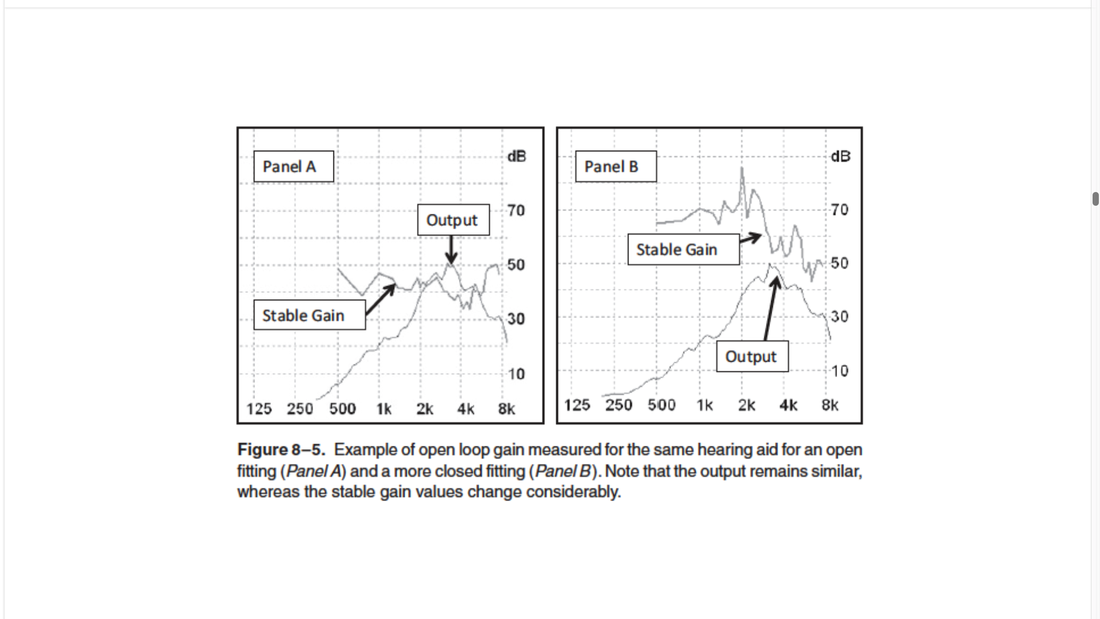
- Examples of real-ear open loop gain measurements are shown in figure 8-5, panel A and panel B
- from the same hearing aid with the same hearing aid setting but using two different types of coupling systems for a patients real ear
- in A when an open custom tip was used, the output of the hearing aid exceeds the stable gain reference by 10dB
- as expected stable gain was the lowest for the frequency region where the output of the hearing aid was the highest
- this is a clear indication that feedback will be present
- hearing aid fitting software can be set so that it will automatically reduce the output for this region and minize the potential for feedback
- this usually is not a wise choice as the patient needs a certain amount of gain in this region for aduibility of speech
- an alternative choice would be to use an earmold with a tighter fit which will serve to increase the stable gain values
- this is shown in panel B
- all parameters of the hearing aid were set the same except in this case, a tighter fitting custom dome was used
- note that we now have the same output peak for the 3500Hz region but we are 5dB below the stable gain values a good probability that we will not have feedback
Ear Impressions
Selecting Hearing Aids and How to Make Choices
- ANL/Acceptable Noise Level
- It is possible to combine speech and noise and have the patient make judgements regarding the signal
- one such measure is the acceptability of the level of the background noise while listening to speech
- this is the design of the acceptable noise level (ANL) test
- relatively new clinical procedure but has been used in research for over 20 years
- Measurement #1 - MCL (most comfort level)
- Measurement #2 - BNL (background noise level)
- running speech set at MCL
- introduce multi-talker babble to maximum level that is deemed acceptable and that still enables the listener to follow that speech passage without becoming tense or tired; determines BNL
- Calculation of the ANL
- MCL - BNL = ANL
- Ex: 72 - 64 = 8
- If patient has a high score, they are at a risk for returning the hearing aids
- COSI - tells you what they value most as a patient, what is most important to get out of process
- The Big 6
- sudden
- ear pain
- unilateral or asymmetric tinnitus
- vertigo
- conductive hearing loss
- otitis media or externa
- EX: if have super bony or super small, tortuous canal, you may not want a cic, would want a receiver in the ear or custom mold
- if exostoses want to avoid having a hard acrylic shell that's in the canal
- Neuropathy - disease causing numbness or weakness
- if have diabetic neuropathy have pain in their hands a lot, may not be able to put in or take out aid
Hearing aid consultation/evaluation
- People will name or prepare people for appointment
- how frequently are they in noisy or complicated environments
- hobbies?
- accessories or assisted listening devices